Welcome
By selecting the Yes, leave Opcaseportalmy.com option you understand that you are leaving the website and that you will be redirected to another Internet site belonging to third parties, for whose content or opinions Amgen Malaysia is not responsible and makes no representations regarding such content or its accuracy. By selecting this option and accessing linked third-party sites, you understand that you do so at your own risk.
The website to which you will be redirected may be designed exclusively for residents of a particular country or countries, as advertised on that website. As a consequence, the website to which you will be directed may contain information on pharmaceutical products or indications that are not approved in Malaysia. If you reside in a country other than the one to which such website is directed, please contact your local Amgen affiliate for the correct information on products in your country of residence.


Case contributed by Assoc. Prof. Dr. Terence Ong Ing Wei, Consultant Geriatrician, Universiti Malaya Medical Centre, Malaysia
Patient Information
Age: 78 years
Sex: Female
Ethnicity: Indian
Comorbidities:
- Type 2 diabetes mellitus
- Hypertension
- Dyslipidaemia
Underlying conditions: Osteoporosis
-
History
- Presented to the Emergency Department in March 2024 with a right inferior pubic rami fracture after slipping in the bathroom.
- Outpatient DXA confirmed osteoporosis (FRAX Major Osteoporotic Fracture: 29%, hip: 15%) and the patient was referred to primary care for management.
- Sustained another fall three months later, resulting in an L1 vertebral fracture.
- There was no Fracture Liaison Service that conducts in-reach into the Emergency Department when she first presented. So, the patient was discharged without the appropriate secondary fracture prevention assessment.
Medication history
- Metformin 1000 mg twice a day
- Diltiazem 60 mg three times a day
- Linagliptin 5 mg daily
- Atorvastatin 20 mg daily
- Gliclazide MR 60 mg daily
-
Investigation
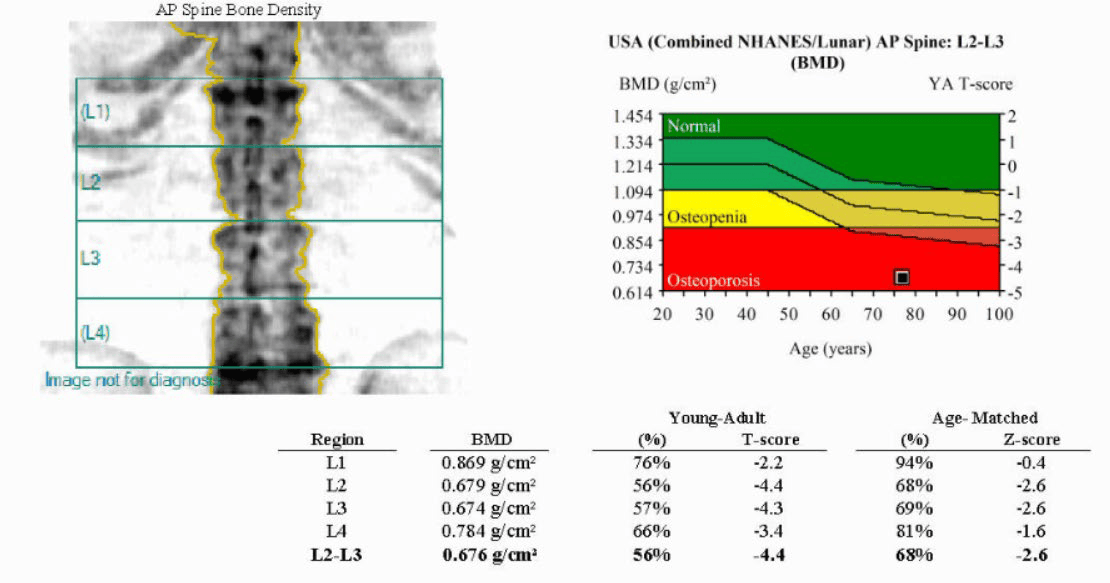
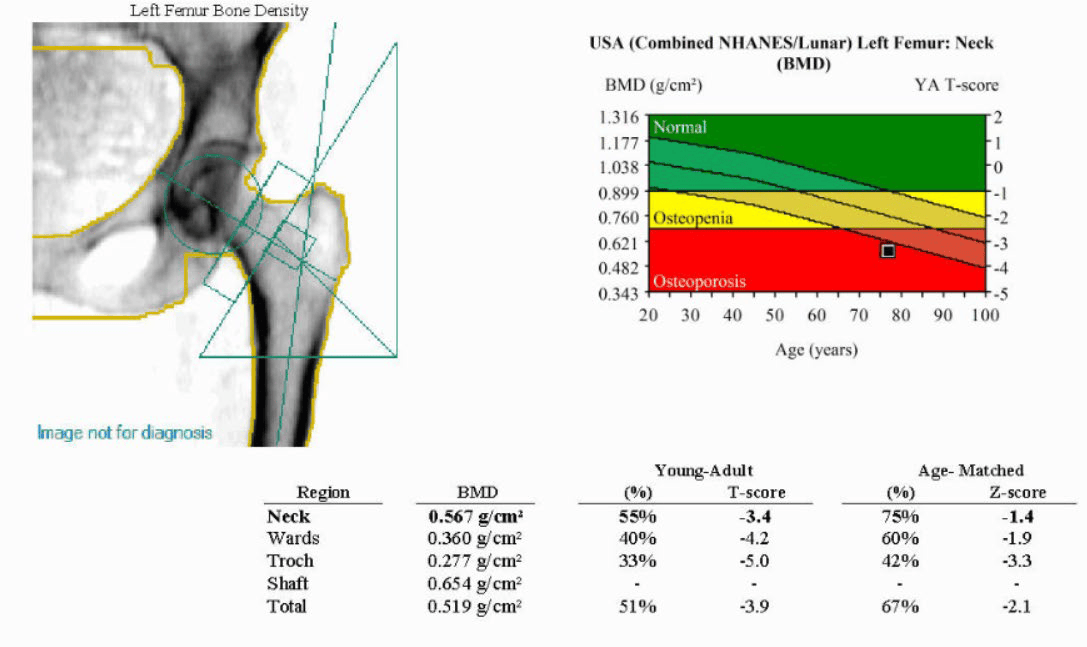
Baseline DXA Scan Results:
- T-score for lumbar spine: -4.4
- T-score for femoral neck: -3.4
- T-score for total hip: -3.9
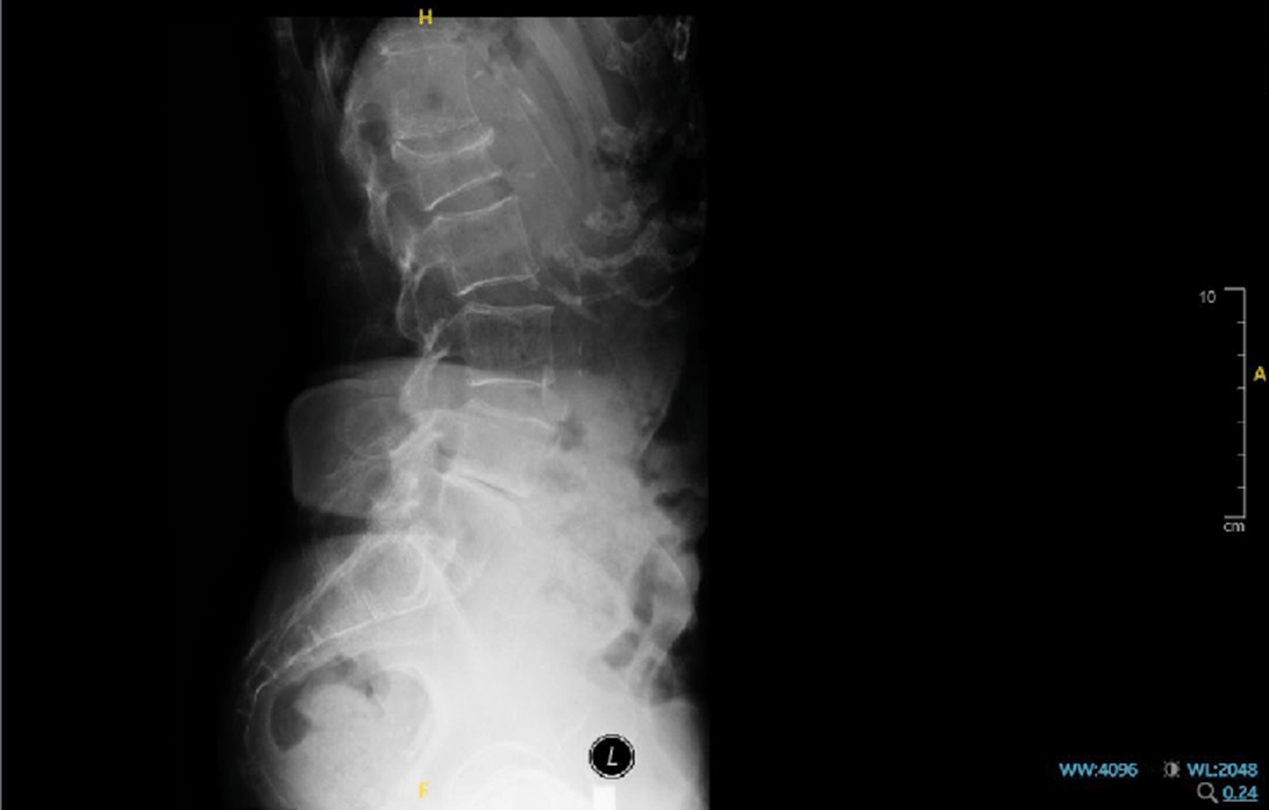
X-ray finding
- L1 fracture is observed
-
Disease progression
- After the two falls, the patient was started on alendronate 70 mg weekly but discontinued after four weeks due to upper gastrointestinal side effects.
- Following counselling and approval for drug subsidy, Denosumab was started about one year later.
- Subsequently referred to the Geriatric Clinic for assessment and identified as very high fracture risk.
- Romosozumab was initiated as anabolic therapy.
- The patient was considered very high risk for further fractures and ideally should have transitioned to an anabolic agent at the earliest opportunity.
- According to Clinical Practice Guidelines. Management of Osteoporosis (3rd Ed.). 2022, she met the criteria for very high fracture risk: sustained two fragility fractures within 12 months, high FRAX hip score: 15%, and a history of injurious or high-risk falls.1
-
Treatment
- Initial therapy:
- Alendronate 70 mg weekly started June 2024
- Discontinued after four weeks due to upper gastrointestinal side effects
- Second-line therapy:
- Denosumab 60 mg SC administered June 2025 (single dose).
- Therapy reassessed following new vertebral fracture.
- Escalation:
- Referred to Geriatric Clinic
- Classified as very high fracture risk under Clinical Practice Guidelines. Management of Osteoporosis (3rd Ed.). 2022:1
- ≥2 fragility fractures within 12 months
- High FRAX hip score: 15%
- History of injurious falls
- Romosozumab 210 mg SC monthly initiated August 2025
- Referred to Geriatric Clinic
- Initial therapy:
-
Summary
- 78-year-old female with recurrent fragility fractures within 12 months and high FRAX scores MOF: 29%, hip: 15%).
- Sequential therapy: Alendronate → Denosumab → Romosozumab, guided by intolerance and CPG-based risk stratification.
- Consistent with MOH Osteoporosis CPG 2022 recommendations for anabolic therapy in very high-risk patients.
-
Reference
1. Clinical Practice Guidelines. Management of Osteoporosis (3rd Ed.). 2022. Ministry of Health Malaysia. MOH/P/PAK/.(GU) –E
Abbreviations
BMD, bone mineral density; CPG, Clinical Practice Guidelines; DXA, dual-energy X-ray absorptiometry; FLS, fracture liaison service; FRAX, fracture risk assessment tool; L1-L4, first to fourth lumbar vertebrae in the lumbar spine. MOF, major osteoporotic fracture; SC, subcutaneous
-
Important Safety Information:Osteoporosis Case BinderThis curated collection of patient case studies aims to provide healthcare practitioners in the area of bone health, with a comprehensive understanding of risk-based treatment approach in the long-term management of patients living with osteoporosis.The patient cases were contributed by bone health experts from respective clinical setting, incorporating evidence-based discussions, guidelines and clinical considerations in the individualised treatment sequencing plans of different real-world scenarios..Please review full product information before prescribingFor Healthcare Professionals Only.Please refer to full prescribing information prior to administrationFor information on Amgen products or to report an adverse event involving an Amgen product, please contact Medical Information at 1800 818 227 or medinfo.JAPAC@amgen.comSC-MAL-CP-00139-Sep2025Endorsed By:
